People are inspiring. Starting in 2014, I would like to profile prominent professionals in the health, safety and construction industry.
The idea originally came from a publication  called, The Synergist,  published by the AIHA. At the back of their magazine they introduce someone in the industry. I have always enjoyed hearing about how others got into this field and where their paths have taken them. Unfortunately, this publication is (mostly) only for people in industrial hygiene. Which (IMO) does little to promote the profession to others outside of it.
Illa Gilbert-Jones, CIH, CSP
How did you get started in IH?
I was in the Masters program at the University of Washington and started out with an emphasis on toxicology. I noticed that those in industrial hygiene in the class before me we’re getting job offers so I decided to also complete the industrial hygiene courses.
What is your background?
My career started at Boeing Company as a safety administrator just before completing my masters. From there I have worked as an industrial hygienist for Bayer Corporation Product Safety for the chemical business, primarily isocyanates. I also worked in their Corporate Safety/Industrial Hygiene group before moving to Phoenix where I worked for Phelps Dodge Mining Company as the Corporate Occupational Health Manager. Although a copper mining company, Phelps Dodge also had smelters, refineries, copper magnet wire, and carbon black facilities with classic industrial hygiene issues-heavy metal fumes. After leaving Phelps Dodge, I did a short stint with Clayton Environmental in California before taking a position with a paint manufacturing/distribution as the Security, Safety, Health & Environmental Manager. After a few years in California, we returned to the Northwest where I worked for SAIF Corporation for over 7 years as a safety management consultant.
You are starting a new position, can you tell us what you will be doing?
On January 1st I accepted the position as Program Administrator for Oregon Fatality Assessment & Control Evaluation (OR-FACE). OR-FACE operates under a NIOSH grant. The program is research based and designed to identify and study fatal occupational injuries. The goal of the FACE program is to prevent occupational fatalities by identifying and investigating work situations at high risk for injury and then formulating and disseminating prevention strategies to those who can intervene in the workplace. More specifically,
• Identify traumatic occupational fatalities through a statewide surveillance network
• Investigate selected traumatic occupational fatalities
• Have a multidisciplinary team analyze the surveillance and investigation data
• Develop and disseminate prevention strategies for these injuries
• Collaborate with other states and NIOSH to develop prevention strategies to decrease the rate of occupational injuries and fatalities
What has been the most satisfying aspect of the field?
Similar to all occupational safety & health professionals, satisfaction is in observing and experiencing improvements in work conditions by reducing risk of contaminant and physical exposures. It is especially satisfying after struggling time-after-time to influence decision makers and then a breakthrough finally occurs and they become safety advocates.
What is the most fun part?
Developing relationships with those as passionate about injury/illness prevention and in giving back to the profession by mentoring those new to the field.
What is the challenging part?
The realization that the job is never done. Serious injuries and fatalities continue to happen. For occupational illnesses from chronic exposure it is very difficult to influence change today for a negative outcome in the distant future.
What advice do you have for those getting started?
Never be satisfied with small changes, be persistent and try all options in pursuing what you believe to be right. Always look for opportunities to increase yours and others in subject knowledge. Additionally, expand your expertise into areas that are normally grouped with industrial hygiene, e.g., safety, risk management, environmental.
What are your hobbies and outside interests?
I try to please my artistic side by learning and writing calligraphy. On the physical side, I try to go to water aerobics regularly, bicycling, and also use a wrist fit-bit to track my daily steps.
What do you see for the future of IH?
Practicing industrial hygiene creates skills for investigating and understanding several layers of causes. These skills enable an H&S professional to critically look at all possible solutions. Because of these skills, I believe industrial hygienists can be successful in a lot of different field. I have seen IH’s become HR Managers, Lab Managers, and of course HSE Managers. The future of IH is taking on more complex issues such as determining true body burden from exposure and in understanding genetic susceptibility to disease from these exposures.
Editor: Thank you Illa! You are inspiring. You may contact Illa directly at OHSU, or at:Â illagjones {at}gmail.c0m

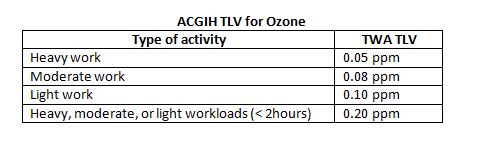 , and the OSHA PEL is 0.1 ppm.
, and the OSHA PEL is 0.1 ppm.





{kind=link}